Definition
Sleeve and bypass are two common types of bariatric surgeries for weight loss. Sleeve surgery reduces stomach size, while bypass reroutes the digestive system. Choosing the right procedure depends on health goals, medical history, and lifestyle.
Obesity is a growing global health concern, linked to diabetes, high blood pressure, heart disease and other complications. For many individuals struggling with weight loss through diet and exercise alone, bariatric surgery offers an effective solution. Among the surgical options, sleeve vs bypass are two of the most widely performed procedures.
Despite their popularity, many people are unsure about the differences between the two. Both surgeries reduce stomach size and help with weight loss, but they work differently and carry distinct benefits, risks, and lifestyle considerations. Making the wrong choice can affect long-term results and overall health.
This article will explain the differences between sleeve and bypass surgery, including definitions, advantages, disadvantages, global trends, recovery expectations and common mistakes. By the end, you will have a clear understanding of which procedure may be best suited to individual health goals.
Quick Overview
| Feature | Sleeve Gastrectomy | Gastric Bypass (Roux-en-Y) |
|---|---|---|
| Procedure Type | Restrictive | Restrictive + Malabsorptive |
| Stomach Size | Reduced by ~80% | Small pouch created |
| Digestive System | Normal pathway | Food bypasses part of stomach and small intestine |
| Weight Loss | 60-70% excess weight in 12-18 months | 70-80% excess weight in 12-18 months |
| Appetite Control | Reduces hunger hormones | Reduces hunger hormones and absorption |
| Risk of Nutrient Deficiency | Moderate | Higher, requires supplements |
| Recovery Time | 2-4 weeks | 3-6 weeks |
| Reversibility | Partial (usually permanent) | Difficult to reverse |
| Ideal Candidates | Moderate obesity, fewer comorbidities | Severe obesity, type 2 diabetes, reflux |
Definition and Explanation
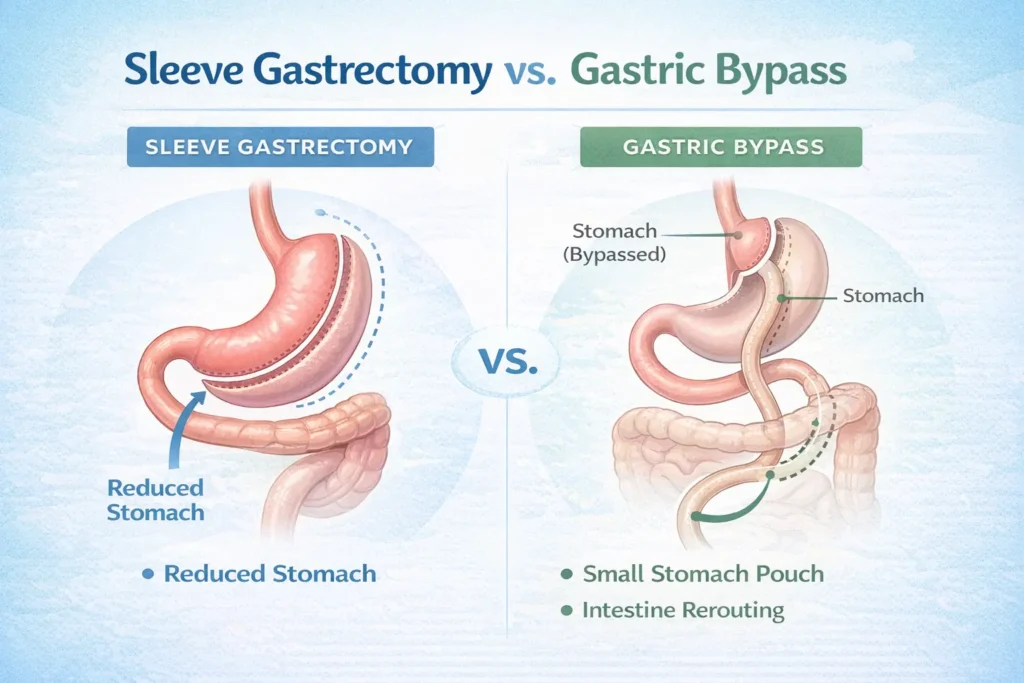
Sleeve Gastrectomy
Sleeve gastrectomy, often called the gastric sleeve, is a restrictive weight loss surgery. In this procedure, about 75-80% of the stomach is removed, leaving a sleeve-shaped smaller stomach. This reduces food intake and also decreases the production of ghrelin, the hormone that triggers hunger.
Patients typically feel full faster and consume fewer calories, leading to significant weight loss over time. The digestive system remains intact, meaning food passes through the stomach and small intestine normally.
Gastric Bypass
Gastric bypass, specifically Roux-en-Y gastric bypass, is both restrictive and malabsorptive. A small stomach pouch is created, and a portion of the small intestine is bypassed. This reduces stomach capacity and decreases calorie and nutrient absorption.
The procedure is highly effective for weight loss and resolving obesity-related conditions such as type 2 diabetes, high blood pressure, and sleep apnea. However, because part of the intestine is bypassed, patients are at higher risk for nutrient deficiencies and must commit to lifelong supplementation.
Advantages and Disadvantages
Sleeve Gastrectomy Advantages
- Less complex surgery than bypass
- Lower risk of complications during surgery
- Preserves normal digestion, no intestinal rerouting
- Reduces hunger by lowering ghrelin hormone levels
Sleeve Gastrectomy Disadvantages
- Weight loss may be slightly lower than bypass
- Not ideal for severe reflux or type 2 diabetes
- Irreversible removal of a portion of the stomach
- Potential for stomach stretching if diet is not controlled
Gastric Bypass Advantages
- Higher average weight loss compared to sleeve
- Highly effective for diabetes and metabolic syndrome
- Can improve or resolve acid reflux in many patients
- Long-term outcomes for obesity-related diseases are well-documented
Gastric Bypass Disadvantages
- More complex surgery with higher risk of complications
- Longer recovery period
- Higher risk of nutrient deficiencies requiring supplements
- More difficult to reverse or revise
Real-World Examples
- Moderate Obesity: Patients with a BMI between 35-40 may prefer sleeve gastrectomy for simpler surgery and fewer complications.
- Severe Obesity or Diabetes: Patients with BMI over 45 or type 2 diabetes may benefit more from gastric bypass due to higher effectiveness in weight loss and metabolic improvement.
- Reflux Considerations: Gastric bypass can improve acid reflux, while sleeve gastrectomy may worsen it in some patients.
- Lifestyle Factors: Patients able to commit to strict diet, supplementation, and follow-up may successfully manage bypass risks.
Data from the American Society for Metabolic and Bariatric Surgery indicates that sleeve gastrectomy accounts for over 60 percent of bariatric procedures in the U.S., while bypass accounts for about 20 percent, largely due to patient preference and risk profiles.
Regional and Global Usage
Bariatric surgery trends vary globally based on healthcare infrastructure, cultural perceptions, and access to medical technology.
North America and Europe
Sleeve gastrectomy is the most common bariatric surgery due to its simplicity and safety profile. Gastric bypass is reserved for patients with severe obesity, diabetes, or severe reflux. Pre- and post-operative care, nutritional monitoring, and follow-ups are highly structured.
Asia
Countries like India, Japan, and South Korea are increasingly performing sleeve surgeries, with gastric bypass used for complex cases. Traditional diets and rapid adoption of western fast-food diets have increased obesity rates, leading to higher demand for surgical interventions.
Middle East
In Gulf countries, obesity prevalence is high, and both sleeve and bypass surgeries are popular. Surgeons often recommend gastric bypass for severe obesity and diabetes management. Post-operative care focuses on lifelong supplementation due to risk of deficiencies.
Latin America
Brazil and Mexico are regional leaders in bariatric surgery, with sleeve gastrectomy preferred due to affordability, recovery, and safety. Gastric bypass is used for severe cases and patients with comorbid conditions.
Africa
Access to bariatric surgery is growing slowly, with centers in South Africa and North Africa offering both procedures. Awareness campaigns and medical tourism from neighboring countries are increasing accessibility.
Globally, the trend is moving toward minimally invasive techniques, improved recovery protocols, and telemedicine follow-ups to enhance patient outcomes.
Common Mistakes
| Mistake | Why It’s Problematic | Correct Approach |
|---|---|---|
| Choosing surgery without medical consultation | Risks complications or inadequate results | Seek professional bariatric evaluation |
| Ignoring dietary guidelines | Can lead to poor weight loss and complications | Follow nutrition plan strictly |
| Not committing to follow-up | May miss nutrient deficiencies or complications | Attend regular post-op checkups |
| Choosing based solely on weight loss | May not address comorbidities like diabetes | Consider overall health benefits |
| Expecting instant results | Weight loss takes months | Maintain realistic expectations and healthy habits |
Exercises with Answers
Exercise 1: Identify which procedure fits the scenario.
- A patient with BMI 38, moderate obesity, and no diabetes.
- A patient with BMI 50 and type 2 diabetes.
- A patient with severe acid reflux.
- A patient who wants a simpler procedure with lower surgical risk.
Answers:
- Sleeve gastrectomy
- Gastric bypass
- Gastric bypass
- Sleeve gastrectomy
Exercise 2: Match benefits to the surgery type.
| Benefit | Sleeve | Bypass |
|---|---|---|
| Reduces hunger hormones | Yes | Yes |
| Significant nutrient absorption reduction | No | Yes |
| Simpler, shorter surgery | Yes | No |
| Resolves severe diabetes | Sometimes | Yes |
| Improves acid reflux | Sometimes | Yes |
Related Concepts and Comparisons
Sleeve vs Bypass vs Adjustable Gastric Band
| Feature | Sleeve Gastrectomy | Gastric Bypass | Gastric Band |
|---|---|---|---|
| Mechanism | Restrictive | Restrictive + Malabsorptive | Restrictive |
| Average Weight Loss | 60-70% | 70-80% | 40-50% |
| Complexity | Moderate | High | Low |
| Reversibility | Partial | Difficult | High |
| Nutrient Deficiency Risk | Moderate | High | Low |
| Recovery Time | 2-4 weeks | 3-6 weeks | 2 weeks |
When to Consider Each Procedure
- Sleeve Gastrectomy: Best for moderate obesity, lower surgical risk, fewer comorbidities.
- Gastric Bypass: Best for severe obesity, diabetes, or reflux.
- Gastric Band: Rarely used today but considered for patients seeking a reversible option.
Prevention and Maintenance
- Follow a post-surgery diet plan and progress gradually from liquids to solids.
- Maintain hydration and take prescribed vitamins and minerals.
- Exercise regularly, starting with light activity post-recovery.
- Attend follow-up appointments to monitor weight loss, vitamin levels, and complications.
- Avoid high-calorie, processed foods to maximize results.
Long-term studies show that patients adhering to post-surgery guidelines maintain 60-80% of their weight loss after five years.
FAQs
What is the difference between sleeve and bypass surgery?
Sleeve reduces stomach size, while bypass reduces stomach size and reroutes part of the small intestine to limit absorption.
Which procedure is better for diabetes?
Gastric bypass is generally more effective at resolving type 2 diabetes.
Is sleeve gastrectomy reversible?
No, it is mostly permanent, as a large portion of the stomach is removed.
Is gastric bypass reversible?
It is difficult to reverse and usually not recommended.
Which surgery has a shorter recovery time?
Sleeve gastrectomy typically has a shorter recovery time than gastric bypass.
Can I regain weight after surgery?
Yes, if dietary guidelines, exercise, or follow-ups are ignored.
Are there risks of nutrient deficiencies?
Yes, especially with bypass surgery; supplements are essential.
Which surgery is safer for moderate obesity?
Sleeve gastrectomy is generally safer and simpler for moderate obesity.
Do both surgeries reduce hunger?
Yes, both reduce ghrelin hormone levels, but bypass may have a stronger effect due to malabsorption.
Can surgery improve acid reflux?
Gastric bypass often improves reflux, whereas sleeve may worsen it in some patients.
Conclusion
Choosing between sleeve gastrectomy and gastric bypass is a critical decision for individuals seeking effective weight loss and improvement in obesity-related conditions. Sleeve is simpler, less invasive, and preserves normal digestion, while bypass offers higher weight loss and metabolic benefits but comes with greater complexity and risk.
Successful outcomes depend on proper candidate selection, adherence to dietary guidelines, lifelong supplementation, and consistent follow-up. By understanding the differences, advantages, disadvantages, and long-term implications of sleeve vs bypass, patients and healthcare providers can make informed decisions for better health and sustainable weight loss.
Discover More Related Articles:
- Outcall vs Incall: Which One Is More Convenient and Why in 2026
- Allograft vs Autograft: Which Option Is Right for You in 2026
- Calm vs Headspace: Which Is Better for Sleep, Anxiety, and Focus in 2026
Jonathan Reed is a dedicated grammar expert and language researcher at TalkNexs.com. With a strong passion for English structure, clarity and effective communication, he has spent years helping students, writers and professionals improve their grammar skills in simple and practical ways.